Spain is rapidly catching up to Italy in terms of both COVID-19 confirmed case and death counts. It has already claimed the top spot as the hottest country in the world with 0.20% of its population infected vs Switzerland at 0.19% and Italy at 0.17%. What is surprising is that Spain did not learn anything from the Italian example and try to avoid the same tragic fate.
Both countries encountered their first confirmed cases on the same day on Jan 31st. Both had several weeks to prepare before the virus took off on its exponential growth but neither was prepared to roll out test kits quickly and widely. The Italians were about 10 days ahead in experiencing exponential growth of the virus. For example, Italy counted 650 cases on Feb 27th, a level above that which led China to quarantine Wuhan, 10 days before Spain crossed a similar threshold on March 8th. Both countries began to institute some travel restrictions then but neither as strong as those imposed on Wuhan. It was not until March 8th that Italy moved to restrict travel nationwide and not until March 23rd that it recommended that non-essential businesses close nationwide. For Spain, these same milestones lagged Italy’s by about a week. This is one reason why Italy is beginning to see early signs of deceleration and possible bending of the curve by next week; while for Spain the confirmed case count is still accelerating and bending of the curve will not happen for at least 2 more weeks.
Perhaps the Spaniards got lulled into thinking that their younger population relative to Italy’s (median age of 42.7 vs 45.5yrs) will save them from the worst of Italy’s tragedy? Certainly, they should not have been complacent about their equally poorly prepared medical systems. Spain’s younger population has allowed them to keep their coincident mortality rate at 8.8% below the horrendous 11.7% observed now in Italy. However, Spain’s slow and weak response could still make them lose more lives than the 12,428 already lost in Italy. Spain’s Prime Minister Pedro Sánchez, hobbled after forming a minority government, did not want to rock the boat and allowed many large events to go forward in March that spread the disease like wildfire.
The lesson here for the US is clear: slow and tepid response will lead to more American deaths than if the President took immediate and strong action to restrict domestic travel. The imposition of incremental travel restrictions is not the answer when slow testing has failed to reveal the true scope of the infection.
The recent debate between Governor Cuomo and President Trump about if, when, and who can or should declare a quarantine around metro-NYC is reminiscent of the debate between Cuomo and Mayor DeBlasio about who should impose travel restrictions around NYC. That 3-day delay will have cost thousands of American lives when the COVID-19 pandemic scorecard is finally tallied. This most recent debate threatens to exact an even greater tribute from the American citizens that these officials all swore to protect.
The epidemic in metro-NYC is out of control and lags the critical timeline that China and South Korea followed. It’s been 16 days since NY crossed the threshold of 500 deaths on March 14th that caused China to impose Draconian quarantines on Wuhan city and then Hubei province. Without strict quarantines, the incremental travel restrictions and social distancing recommendations have helped a little but it was not until Cuomo announced statewide shelter-in-place rules on March 20th that the free-flowing coronavirus finally slowed its rampage through the entire metro-NYC area. The slowness to act allowed much of NJ and certain portions of CT to become heavily infected. The infection now needs to be managed on a tri-state basis and only full cooperation between the Mayor, the Governors, and President Trump can really work to contain the wildfire. And yet they are wasting time bickering about who gets to captain this listing ship.
Governor Cuomo should be commended for quarantining New Rochelle, NY. However, it turned out to be too little, too late because under testing led him to draw a box that was too small — the infection had already spread beyond the boundaries of New Rochelle. Until wider testing is completed, a general quarantine with wide enough boundaries is the only way to stop the virus in Metro-NYC and shield the rest of the country. NY state has made some progress in ordering wider testing of its residents so that now 0.9% of New Yorkers have been tested for the virus, the best of all states in the US — matching the thoroughness of South Korea. But NY needs to do more because more of its citizens appear to be infected than in South Korea. Currently, 0.31% of NY residents have been infected whereas only 0.02% of South Koreans have been infected. Testing is way behind where it needs to be in NJ and CT where only 0.4% and 0.3% respectively of their population have been tested. Without wider testing, the only solution is to quarantine the entire metro-NYC area. After testing expands further and we can gain more confidence that every infected person and their contacts in the metro-NYC has been identified we can then transition to a more targeted quarantine where only those identified as confirmed and suspected are ordered to stay in 14-day quarantines.
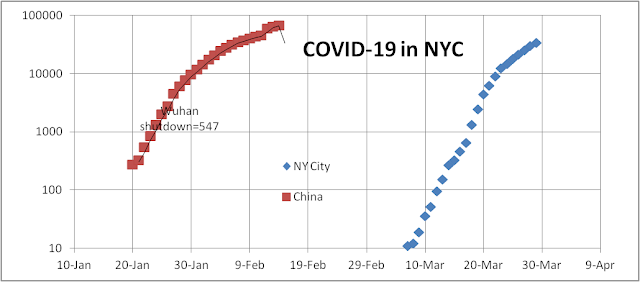
The graph below shows the rapid exponential growth in confirmed COVI-19 cases in NYC compared to China. But it also appears to show that the doubling time in NYC has slowed to 4.3 days, but part of this slowdown has been due to the temporary bulge in cases in the prior week due to catch up testing. If NYC broadened the testing protocol this curve might accelerate again as we count milder and asymptomatic cases. This week’s data should allow us to tell whether the infection rate has slowed for real or not. If nothing is done the virus is certain to produce more infections (33,768 as of 3/29) and more deaths (678 as of 3/29) in NYC than all of China. This would constitute an avoidable tragedy greater than 9/11 that the mayor, the governors, and the president will all live to regret.
Testing early, quickly, accurately, and thoroughly is important in the war against COVID-19. Not only does it allow us to identify those who have been infected early in their infection, it allows us to track all their contacts more thoroughly, it allows us to treat them more effectively, and it also allows us to restrict their travel and isolate them before they have a chance to infect others (the 4T program to fight epidemics). All 4 steps are necessary to allow a country to effectively control its epidemic at minimum cost to society. Countries that have effectively adopted this program such as South Korea and Singapore have been able to control their epidemic without resorting to Draconian measures such as those employed by China who quarantined entire cities and provinces because they didn’t know the full dimensions of their problem.
On this score, the US has done very poorly — starting slowly, with numerous setbacks and a far too restrictive set of test protocols. Testing was impeded in February by several CDC errors including the requirement that they verify all testing results centrally. Testing improved significantly after the CDC removed this bottleneck toward the end of February and permitted private testing labs to do testing. Since then the number of tests completed (top line in the graph below) has grown exponentially to keep up with the exponential growth in infection (positive results in the graph below). A good sign but not ideal.
Ideally, you want the number of tests performed to be significantly greater than the number of positive cases that you suspect is in the population to make sure that you are counting every infected person. As of yesterday, 3/28, the US has tested just 0.2% of its population. By comparison South Korea reached this milestone on 3/1 and has now tested 0.8% of its population. 2.4% of its tests came back positive while 15.9% of US tests came back positive. Unless we have good reason to believe that our underlying infection rate is really 15.9% we could still be under testing by a factor of 6.5. So we are doing better but not good enough.
Under-testing is a critical problem because unless we have an accurate count of the true number of infections we may be over-estimating the mortality rate or deadliness of COVID-19. In February, the measured coincident mortality rate {deaths (see the fourth line in the graph above) divided by positive cases} was as high as 8% on 3/3 because the denominator was biased too low. As we tested more the denominator grew faster than the numerator and this coincident mortality rate fell to near 1%. This, however, was biased too low. As we had pointed out before, it takes -1 to 21 days for diagnosed cases to result in death or cure (-1 for many cases diagnosed after death), with most taking 3–7 days with a median of 5 days yielding our lagged5 estimate of 4.5% for the US.
Not every state has tested with the same degree of rigor. The table below ranks the states by its hotness measure — i.e., the number of confirmed cases per million population. The testing metric in the last column show how thoroughly each state has tested its population and how likely or unlikely its results are biased. On this score NY and WA have done the best and NY mortality rates are least likely to be biased. WA estimates are probably biased too high because of the source of their infection in a nursing home bias the age of their dead too high to be representative of the state. On the other end, California had some of the earliest cases in the country but their testing has lagged. They have a huge number of pending cases that should be resolved soon and improve the accuracy of their numbers but even then they would still be much worse than NY and WA. Our guess is that California’s confirmed case count is way too low.
One final note, the third line in the graph above shows the number of cases serious enough to require hospitalization. Many of these cases will end up in the death count whether any drastic action is taken tomorrow or not. They serve as a leading indicator of future problems if they soar out of control and overwhelm the capacity of our hospitals. That they are growing exponentially is not a good sign.
Florida Governor DeSantis has failed to recognize the seriousness of the exploding COVID-19 pandemic in Florida. His slow response and poor judgment have already cost many Floridians their lives and may cost many thousands more if he fails to act now.
State
Infections /million
Infections
Deaths
Mortality Coincident
Mortality Lagged5
NY
2,361
45934
604
1.3%
3.6%
NJ
994
8825
108
1.2%
5.1%
LA
591
2746
119
4.3%
12.7%
WA
486
3700
175
4.7%
8.8%
MA
466
3240
35
1.1%
5.1%
MI
366
3657
92
2.5%
8.4%
CT
362
1291
27
2.1%
8.2%
CO
301
1734
31
1.8%
5.3%
IL
239
3026
34
1.1%
3.3%
GA
207
2198
65
3.0%
9.3%
FL
191
3198
46
1.4%
4.7%
PA
173
2218
22
1.0%
4.1%
CA
121
4791
94
2.0%
5.3%
Among the 50 states in the US, Florida currently ranks 11th in hotness — i.e., the number of confirmed cases per million residents with 191 (see the second column in the table above). Not so bad until you realize that every state hotter than Florida (other than Georgia) has already ordered statewide travel restrictions of one form or another. In fact, 25 governors to date have ordered some form of lockdown. DeSantis has refused to hear pleas from his legislators to do just that. So Florida mayors and county commissioners have taken the matter into their own hands and ordered travel restrictions on a county-by-county basis. For example, in the Metro Miami area, both Miami-Dade and Broward counties have travel restrictions in place. In the metro Orlando area, Orange County has travel restrictions but Seminole County does not. This has led to confusion and ultimately will result in ineffectiveness because so many people work, live, shop and travel back and forth across both counties. These travel restrictions must be enacted on an MSA (metropolitan statistical area) or a state level to be effective.
Governor DeSantis’s slow response is one thing, worse is his open invitation to Spring Breakers to effectively “come on down and party, the water is fine.” Florida currently has a patchwork of rules regarding beaches — some are open, some are closed, some are open one day and closed the next. New Orleans has just realized the folly of their actions in allowing Mardi Gras to proceed this year at the end of February. Two weeks later it has resulted in an explosion of cases in New Orleans and Louisiana (#3 in hotness in the table above). The same fate could await Florida a few weeks after Spring Break ends. Along with bikers from Bike Week, returning Snowbirders from metro-NYC, Florida Governor’s slow and weak response could cost many lives. Florida was COVID-19 free before March 3rd (although we have serious doubts about this given severe under-testing nationwide and in Florida), and this pandemic need not have happened in Florida if Trump and/or DeSantis had acted in February. With the pandemic growing exponentially in Florida (see log-linear graph above), it is still not too late to act now and save thousands of lives in Florida.
Since March 9th when we posted our first story on COVID-19 and made our call for quick and decisive action to stop the virus in the US, the story has worsened considerably. The US now leads the world in confirmed COVID-19 cases with over 85,000 — surpassing China, Italy, and Spain. Worse, there is no sign that the US pace of infection is slowing anytime soon whereas China’s infection has been under control for several weeks and they are letting workers go back to work in all areas of China outside Wuhan. China’s risk from the pandemic is not over because with the virus spreading globally they need to be ever vigilant about re-infections. But their early draconian travel bans and their thorough testing, tracking and treatment of all potential infectees have allowed them to suppress the pandemic.
The virus is continuing to grow exponentially in the US with a doubling time of about 3 days (see figure above where day 0 is Jan 11th when the world got the genetic code for the novel coronavirus and could begin to attack the enemy). In the meantime, the President is still hoping to remove currently lax travel restrictions by Easter. This wishful thinking is criticized by all respected scientists. With the confirmed case count heading past 100,000 by tomorrow this is not the time to ease up on the fight, but the time to institute strong domestic travel restrictions and wider testing. The first 100,000 confirmed cases in the US achieved tomorrow will have taken 66 days, the next 100,000 could be confirmed in 4 more days by month-end — all with the US still under-testing!
For NY state residents who are at the new epicenter of this global pandemic, the risk is especially acute. The infection rate is 2 per 1000 NY residents so if you contact just 5 persons per day (the current congregation guidance limit) your chance of getting infected is 1%. In certain parts of NYC (e.g. Westchester County) the infection rate is even higher at 6 per thousand. Over the course of the next few weeks as the infection continues to rage each person’s chance of getting infected will be increasingly higher.
NYC is not the only hot spot in the US: Seattle, San Francisco, New Orleans, Miami, Chicago, Atlanta, and Detroit are all above the level of infection when China quarantined Wuhan. This means we are weeks behind where China was able to limit their death count to 3,300. In fact, the death toll in the US will be much higher: with a case count of 85k+ and an estimated mortality rate of 4.7% — 4000 deaths are already baked into the US. forecast. Further, with the infection progressing exponentially the final death count will be much higher.
22 governors in the US have already instituted some sort of travel restrictions, and their residents will be better off for it in the long run. For those less fortunate in Florida and Pennsylvania, the most infected states without a state-level travel ban, they will have to wait for their governors or President Trump to wake up and recommend national travel restrictions rather than remove the weak ones currently in place. A national travel ban coordinated by the President makes the most sense since the risk of re-infection will always be high if a few states decide not to impose travel bans.
It’s not too late yet. This could all be over in a couple of months if Trump and the government take decisive action regarding wider testing and travel restrictions now. If not, maybe herd immunity will end this after a few hundred thousand Americans die.
Switzerland’s response to the COVID-19 pandemic has been rather tepid compared to those of many other countries in Europe. Its slow and weak response may be partly due to its Federal structure with a weak central government. The Federal Council’s latest proclamation on March 20th was to announce no lockdown but an incremental tightening of congregation limit to less than 5 persons whereas Germany has lowered a similar limit to 2 persons. Its basic attitude has been to let the coronavirus have free rein and spread and now it is #1 in hotness of all populous countries in the world, with 1,222 confirmed cases per million citizens — surpassing its neighbor, Italy. Part of the problem has been its insistence on maintaining open borders and its historical “neutrality” in many wars. But the coronavirus is an invader of a different sort — totally unsympathetic to neutrality.
Country
Infections /million
Infections
Deaths
Mortality Coincident
Mortality Lagged5
Switzerland
1,274
10,897
153
1.4%
2.8%
Italy
1,141
69,176
6,820
9.9%
15.9%
Spain
1,018
47,610
3,434
7.2%
15.9%
Norway
530
2,868
13
0.5%
0.7%
Germany
406
34,009
172
0.5%
1.1%
France
342
22,304
1,100
4.9%
10.5%
Iran
323
27,017
2,077
7.7%
10.6%
Denmark
296
1,715
32
1.9%
2.7%
Sweden
227
2,286
36
1.6%
2.7%
S. Korea
177
9,137
126
1.4%
1.5%
U.S.
166
54,968
784
1.4%
4.6%
UK
119
8,077
422
4.9%
11.3%
China
57
81,218
3,281
4.0%
4.1%
Fortunately, its lagged5 mortality rate (the current death count divided by the average confirmed cases 3–7 days prior) has been a low 2.8% compared to 15.9% in neighboring Italy where many of its infections came from. Partly this has been due to the lower median age of 42.4 versus 45.5 in Italy. Partly it has been due to a slightly better hospital bed situation. But we predict that with such a high infection rate, the Swiss healthcare system will soon be overwhelmed and higher mortality rates are very likely. Someone should be sounding the alarm in Switzerland. Neighboring EU countries should be very concerned since the Swiss hot zone may reinfect them even after they were able to control their own country’s pandemic.
Americans love Italians but no one wants to follow the fate of the Italians in their encounter with COVID-19. More Italians, 5,476, have died of COVID-19 in just the last month than any other country in the world by far. China is second at 3270 total to date. Scaling this 29 days rate to a year, it would mean 68,900 deaths for a country with a population of 61M. This is a worse rate than the 153,200 Italian civilians that died over 6 years in WWII.
And there is very little sign that the curve has peaked (see figure below). The number of active cases has risen to 46,638. This has overwhelmed the health care system in many parts of Italy resulting in the highest mortality rates in the world, 9.3% (coincident). Our best guess lagged5 rate is a horrendous 17%. Aside from an overstressed health system where a scary high 31% of all hospital beds in Italy on average have been used to treat COVID-19 victims, Italy also has one of the oldest populations with a median age of 45.5 years contributing to the high mortality rate. Given this high mortality rate and number of active cases, we project that another 8,000 Italians will die in the next few weeks no matter what they do — very, very sad.
So where does one look for a ray of sunshine in this dark winter that has just passed? In both China and South Korea where the virus has been “controlled” – stringent travel restrictions were imposed and then the curve turned 3-4 weeks later. In Italy, the upgraded travel restrictions including closing the borders were put into place on March 8th and we expect improvement by the end of this month or early in April. Expect means little with a pandemic that has shocked the world with surprises and new records set almost every day. However, if you look at the graph of active COVID-19 cases in Italy, you can see that yesterday’s data suggest a bend in the curve could arrive in a week or two. While the number of active cases increased by 2,957, the rate of increase dropped below 10% for the first time in 10 days. This shows that the number of active cases could soon stop rising at an accelerating rate — a necessary pre-condition for peaking. We cannot be really optimistic until we see a true turn — when the number of resolved cases (recoveries plus deaths) per day exceeds the number of new cases as they have in China and South Korea. This milestone would mean that the count of available hospital beds would finally increase after a month of decreasing capacity. The first signs of spring may arrive soon in Italy.
A second reason for optimism is that a report emerged this week that a town of 3,000 in Italy was able to eradicate the coronavirus in an experiment that called for widespread testing that resulted in zero new cases this past week. We have always called for early and thorough testing, tracking, and treatment (TTT) as a necessary condition to combat a pandemic. We did not know that when combined with strict travel restrictions (TTTT-4T approach) they would be sufficient to eradicate the virus from a city, region, or country. But this is essentially what the South Koreans have been able to do. They have controlled the virus infection and are working toward virus-free status. As long as they remain vigilant against foreign re-infection they can achieve zero cases from both domestic and foreign sources. It would be important to replicate this approach with a proof of concept test for a Western city of size, for example, San Francisco. Trump, with his war powers, can order all American companies with test-kit manufacturing capacity to make millions of test kits or purchase them from foreign suppliers in the coming days for this test. If Trump fails to do this we will have to appeal to private institutions such as the Gates Foundation. The virus has spread widely in the Bay Area, but if they test everyone and apply this Italian 4T approach and demonstrate that it works, If more test-kits can be made or bought in the next week, we can immediately apply this 4T approach to metro-Seattle and metro-NYC which has become the new epicenter of coronavirus infections in the world. Americans should be ready to follow this Italian model in the war against the coronavirus. Then, all the Italian suffering would not have been in vain.
Is there any light at the end of this dark tunnel that is not the headlight of an oncoming train?
There are some glimmers of hope in the data from China and South Korea where they seemed to have successfully “controlled” their COVID-19 infection. This does not mean that they have no new cases and certainly does not mean that they have no more deaths. It just means that they have flattened the curve, and reduced the number of active cases in their country. The number of net new infections — i.e., the number of confirmed cases minus the number of resolved cases (deaths plus cures) — is an important statistic to track (shown in the last column in the table below).
The number of net new infections is an important statistic to track because it tells us whether the situation is likely to get out of control. If this number is increasing every day the country might run out of hospital beds and doctors and lose their ability to treat every patient well. If this number plateaus or decreases it means that enough patients leave the system to allow new patients to be handled properly. For China, this statistic turned negative on Feb 18 when the number of newly recovered and dead exceeded the number of newly infected. This occurred 26 days after they locked down Wuhan and Hubei Province. For South Korea, they flattened the curve on Mar 11th, roughly a month after their infections started to accelerate in mid-February. For some countries like Singapore, Taiwan, and Hong Kong they seemed to have been able to control their infections for periods of time. However, as COVID-19 has spread globally, these countries have experienced periods of re-infection from international travelers.
The other important “good news” is that the basic underlying mortality for COVID-19 is closer to 1% rather than the WHO estimate of 3.4%. The table below summarizes the data for China, South Korea, and Singapore and gives their infection rate per million citizens, the total infections experienced to date, the total death count, and the mortality rate estimated three different ways: using contemporaneous data, using time-lagged data, and using resolved case data. The coincident mortality rate is the easiest to calculate for all countries and merely takes the total death count and divide it by the cumulative number of confirmed cases. For a rapidly spreading infection, this estimate is always too low but for a mature outbreak, this estimate is more correct. This lagged5 mortality rate is calculated as the death count divided by the average case count 3–7 days prior. In general, it takes about that amount of time for a confirmed diagnosis to result in death. For outbreaks that are near the end, we can just look at the final death count and divide it by the total cases resolved. For China, all three estimates are very close to 4.0% with the resolved case estimate falling slowly toward 4% as more patients finally get released from the hospitals. This rate for China is high due to the disastrous situation in Wuhan where the health care system was overwhelmed. The mortality rate in the rest of China is closer to the base mortality rate of 1% experienced by other countries whose health systems were able to keep up with the infection spread. You can see in South Korea the mortality rate estimate has held steady near 1% for weeks. They also have one of the best health systems in the world in terms of hospital beds per capita –1.2%. Singapore has had no deaths for about 2 months and even after reporting their first two deaths yesterday they still show a reasonable low mortality rate, albeit with large statistical errors.
Country
Infections /million
Infections
Deaths
Mortality Coincident
Mortality Lagged5
Mortality Resolved
Net New
China
57
81008
3255
4.0%
4.0%
4.3%
(556)
S. Korea
170
8799
102
1.2%
1.2%
3.8%
(240)
Singapore
67
385
2
0.5%
0.8%
1.4%
36
In our opinion, the prescription for success in the COVID-19 fight — measured in terms of limiting the total number of death per million citizens — is:
Test, track, and treat every possible case immediately — US
Enforce strict travel restrictions and social distancing rules immediately
Endure one month of hardship until the curve turns — Italy
Endure another month of more bad news regarding high infections and deaths — South Korea
Be sure to vigorously attack re-infections — China, Singapore, Taiwan, HK
Light at the end of the tunnel with just 1% of those infected dying over the next 2 months — better than the millions currently projected for the US with little action.
Now it turns out that many people in Trump’s administration and the senate (Richard Burr, Kelly Loeffler, James Inhofe, and Dianne Feinstein) were warned as early as late January that COVID-19 could evolve into a pandemic. Rather than using this information to prepare the country with a detailed plan for testing, tracking, and treatment of potentially millions of Americans, they used the information and the time to sell their stocks and line their own pockets. Further, rather than telling the truth to the public and possibly jeopardize their ability to short stocks in time, they told the public that Trump had everything under control and that everything would turn out fine. Trump himself claimed multiple times that the quarantine against China was working and that President Xi was doing a great job managing the coronavirus epidemic. He claimed the situation was under control and no one needed to worry.
This inaction and duplicity could end up costing America hundreds of thousands of lives. If they had developed a solid plan to defeat the coronavirus and put it into place in early February, the epidemic could have been stopped before it gained traction in mid-February in the US. At that time we only had 15 confirmed cases. The epidemic could have been avoided for not only the US but possibly for other countries around the world The US used to exhibit moral, ideological, and scientific leadership that other countries followed. We cautioned about climate change and pushed for environmental protection programs and convinced others to follow. If we had a solid solution in place by mid-February other countries could have adopted our plan and also controlled their own infections in time. There might not have been any need for the WHO to declare a pandemic on March 11th. Millions of deaths and trillions of dollars of economic opportunity lost could have been avoided.
What makes their actions especially appalling is that they could have kept their stock investments or added to them on the assumption that Americans were fully capable of finding the solution to the new epidemic and the stock market would have kept on rising. That they had so little faith in their own abilities and that of their fellow Americans to solve this problem is beyond sad. If it turns that after a thorough investigation of these stock sales that this was just a highly improbable coincidence, we apologize for being critical.
Previously, we had looked at the Scandinavian countries (Norway, Sweden, and Denmark), Germany and Austria who seem to be faring better than average to see if we could then find some best practices to improve our fight against COVID-19. Other smaller countries such as Singapore, Taiwan, and Hong Kong should also be examined for best practices but they may be less applicable given their much smaller size and structural differences from us. However, we made the additional argument that if the US adopted a divide and conquer approach and broke the big problem (US) down to smaller and more manageable regions (MSAs), the smaller country best practices may then be examined and adapted. Finally, South Korea should be singled out for their excellent performance – they have their outbreak under control in record time with a very low overall mortality of 1.1%. Their early and decisive response as well as their excellent healthcare system (12.27 hospital beds per thousand population) served them well.
Today we want to focus on the other half of the coin: countries that are clearly faring worse than average and see what we can learn not to do. Italy is the prime example whose death count surpassed that of China today. Clearly, our hope is to avoid becoming another Italy – it would be a disaster that the US may take decades to recover from. Italians are handicapped by two major shortcomings: a significantly older population especially in Northern Italy where the infection started, and (2) an inadequate amount of hospital beds per million population of 3,180 that quickly got overwhelmed. Moreover, their very sociable citizenry did not adopt social distancing quickly and forcefully. One caveat, the measured mortality rate may be higher than the actual mortality rate especially for countries with overwhelmed health systems because they fall behind in testing and less serious cases do not get counted as confirmed cases increasing the apparent measured mortality rate. This early indicator may need to be adjusted after the peak infection has passed and the infection controlled.
Country
Infections /million
Infections
Deaths
Mortality Coincident
Mortality Lagged5
H Beds /million
Median Age
Italy
677
41,035
3,405
8.3%
16.0%
3180
45.5
Switzerland
483
4,133
43
1.0%
2.7%
4530
42.4
Spain
386
18,077
831
4.6%
12.8%
2970
42.7
Norway
331
1,790
7
0.4%
0.6%
3600
39.2
Iran
220
18,407
1,284
7.0%
10.2%
1600
30.3
Denmark
199
1,151
6
0.5%
0.7%
2610
42.2
Germany
183
15,320
44
0.3%
0.9%
8000
47.1
France
169
10,995
372
3.4%
8.1%
5960
41.4
S. Korea
166
8,565
91
1.1%
1.1%
12270
41.8
Sweden
143
1,439
11
0.8%
1.2%
2220
41.2
China
57
80,928
3,245
4.0%
4.0%
4340
37.4
UK
48
3,269
144
4.4%
17.4%
2500
40.5
U.S.
40
13,289
183
1.4%
6.0%
2770
38.1
Italy is not the only country with a cautionary tale to tell. Others that appear to have double-digit mortality rates include Iran, Spain, and the UK.
Iran is in a unique situation and no one seems to be 100% sure of their data. We calculate a best guess lagged5 mortality rate of 10.2%, but suspect that they are hiding the full extent of their sorrows — burying their dead in huge unmarked trenches. They do have the benefit of a very young population with a median age of 30.3 years — the lowest of all the countries we are tracking. Two shortcomings far outweighed their relative youth: (1) an unwillingness to accept the truth until it was too late to act and (2) a poor healthcare system with only 1600 hospital beds per million population which clearly got overwhelmed.
Spain has a lagged5 mortality rate of 12.7%. They really had few excuses not to react more forcefully sooner. They encountered their first case on January 31, the same day that Italy did. And they were additionally fortunate that the outbreak did not become serious until February 25th, nearly 4 weeks later. Spain, along with other EU countries could have been saved if they dropped the EU open border policy during that period and enforced strict travel restrictions. They did not have to let their infection run amok. Now their future looks as bleak as that of Italy. Their hospital bed count is similar to Italy while their median age is younger than Italy’s. They did not take advantage of their forewarning.
Finally, the UK is another infection that need not have run amok with a mortality rate did not have to be as high as 17.4%, a lagged5 estimate that is worse than even Italy’s. Much of the blame can be laid at Boris Johnson’s feet who decided that it was OK to adopt the “herd immunity” concept for humans. This essentially argued that it was OK if they did nothing since after a while the remaining population would have enough people with immunity that the pandemic would stop by itself. Those who survived would make for a stronger herd. As soon as people realized that this is what the government was doing they rebelled and the government had no choice but to act. To be generous, more likely they did not act quickly and when questioned searched for a viable theory for their inaction and then decided oops the theory sounded too brutal. It really doesn’t matter – they acted way too late. Now their low hospital bed count of 2,770 per million will negatively impact their mortality rate.
One fatal mistake that all these high mortality countries made is recognizing the problem too late and reacting too timidly. Unfortunately, these are two mistakes we have already repeated in the US.







{kind=link}