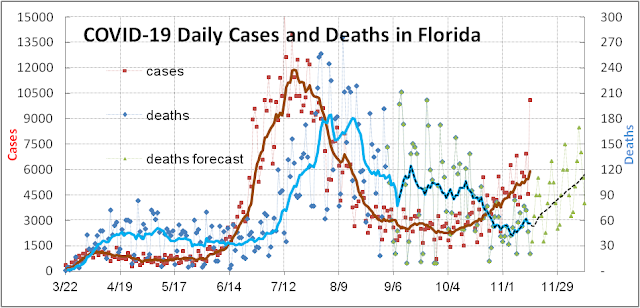
COVID-19 cases in the USA have shown a sharp decrease over the last 8 days causing the 7-day rolling average to peak and rollover (see figure below – red squares). The question is whether this is measuring a real lasting phenomenon – perhaps attributable to local COVID-19 fires burning out, or to mitigation factors taking hold, or to some temporary factor associated with the Thanksgiving holiday. The answer is probably a combination of all three that will ultimately be overwhelmed by an increase in Thanksgiving transmission.

Some COVID-19 outbreaks have burned so strongly and for so long (3-4 months) that local “herd immunity” may be acting as a retardant to the fire. For example, in North Dakota (ND) 10.3% of the population has now been confirmed infected (see table below).
| State | Confirmed | Testing | Est. Pop | Deaths | Death per | Fatality |
| Infection % | Positive % | Infection % | million | |||
| ND | 10.3 | 23 | 47 | 920 | 1,207 | 1.2 |
| SD | 9.0 | 24 | 44 | 943 | 1,066 | 1.2 |
| IA | 7.2 | 19 | 27 | 2,400 | 761 | 1.0 |
| WI | 6.6 | 15 | 20 | 3,307 | 568 | 0.9 |
| NE | 6.5 | 17 | 22 | 989 | 511 | 0.8 |
| UT | 6.0 | 9 | 11 | 868 | 271 | 0.4 |
| USA | 4.2 | 7 | 15 | 273,077 | 825 | 2.0 |
Given their low testing rate and associated high positivity rate near 23%, the true underlying infection rate could be 5X to 10X higher than reported (higher positivity rates correspond to a higher hidden population of infectees). This means that ND could have passed the “herd immunity” threshold of 60%-70% estimated by most epidemiologists. South Dakota (SD) is not far behind at 9.0% confirmed with 24% positivity rate. Six US states (ND, SD, IA, WI, NE, UT) are already above 6% confirmed infection rate and could be approaching the herd immunity threshold in a few months. Four of these states (ND, SD, IA, NE) has refused to impose any kind of statewide mitigation measures and avoided testing and thus have a high hidden population of infectees. Hundreds of counties in the USA could be approaching this threshold. These states and counties could well reach herd immunity before vaccines become widely available in March. By then it would be too late for vaccines to save lives already irretrievably lost.
Letting the virus run wild has come at a great price for the Dakotas. Both states have now joined the unenviable 0.1% club, that is more than a thousand deaths per million population reached by 10 USA states and only 3 countries in the world: Belgium, San Marino, and Peru. (For reference the USA as a whole is at #10 in the world with 825 deaths per million. The USA as a whole is far from herd immunity with just 4.2% of the population confirmed infected and an estimated 15%-20% as the true underlying infection rate.)
Part of the reason for the recent topping of case counts could be due to the wide range of mitigation measures many counties and states have undertaken recently to flatten the curve and deal with the overwhelming demand for healthcare services (current hospitalizations are 56% higher than ever before in the USA). These measures include mask mandates (which we view as the cheapest mitigation measure), limitations on assembly, curfews, and business/activity shutdowns. Many of them could take several weeks to cut transmission and to manifest themselves in the data. Moreover, many of them are not mandatory and depend on widely varying voluntary compliance. Given the wide spectrum of responses, it will take some time to sort out which has been effective and which have not.

Finally, part of the reason for the recent dip in cases could also be just a matter of timing. Many young adults including college students got tested for COVID-19 in the days before Thanksgiving, hoping to get negative results and a pass to go home (see graph above). This raised the number of tests conducted to a record high of 1.98 million tests in the USA on Nov 21st. 91% of these tests came back negative and gave millions “pass” to travel. Over the last 8 days, the number of tests dropped to 1.28 million on Nov 29th – much of it due to many Americans taking long weekends off for Thanksgiving. We expect reported tests, cases, hospitalizations, and deaths to increase again soon.
The incoming Biden administration must take charge of the pandemic war immediately. We are forecasting that an additional 74.5k Americans will die over the next 4 weeks due to cases and hospitalization already in the pipeline. Moreover, every day’s delay over the next 51 days will add 2k-3k to the death toll (this mean >100k lives irretrievably lost before Inauguration Day and vaccine public availability) – an avoidable and unforgivably tragic chapter in American history.