The new US administration has made re-opening schools a priority. There are many benefits to re-opening schools and certainly, re-opening schools are more important than re-opening bars and many other businesses. But there are many risks as well.
One of the risks is the susceptibility of kids to COVID-19. Kids suffer far fewer fatalities and hospitalizations than older adults (although kids could suffer long term ill effects with COVID-19). The question really comes down to how easily do kids acquire the virus and how easily do they transmit COVID-19 to others and fuel the pandemic.
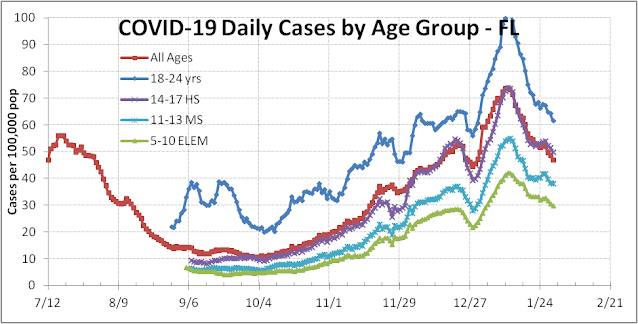
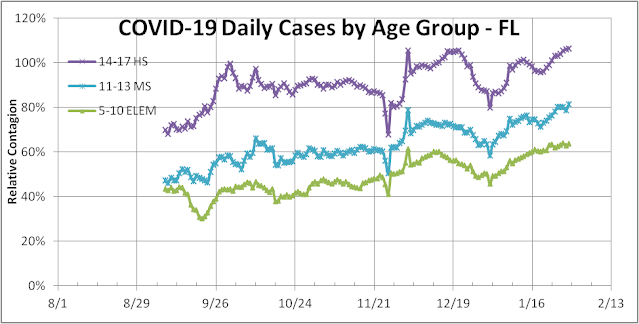
In Florida, most schools and universities reopened in late August 2020. Since then the number of daily confirmed cases per capita has risen steadily for all age groups. College and university-aged (18-24yrs) students are most active and mobile and show the highest cases per capita – currently 30% above average. High school students (14-17yrs old) have always tracked near the average infection rate. Elementary school student (5-10yrs old) infection started out near 30% to 40% of average but has risen steadily over the last 5 months. Currently, they are 64% as contagious as the average Floridian, and middle school students are 81% as contagious (see graph below).
Why have kids become more contagious?
1. One explanation is that with school reopening, kids are tested more often. While testing has increased, the positivity rate has gone up as well reflecting a real increase in community spread. Over the last 7 weeks, tests have topped out at 100k/day in FL.
2. The spread of more contagious variants from the UK, South Africa, and Brazil has increased the rate of transmission, including among kids. Whether kids are more susceptible is an open question. FL data suggest that kids may be.
Re-opening schools should be done in phases with K-5 grades re-opening first and perhaps high schools not at all until community spread is much lower than it is today. In Florida, most high schools have re-opened along with most sports and this has exacerbated outbreaks in Florida. We strongly discourage high contact sports such as high school wrestling that have led to super-spreader events.
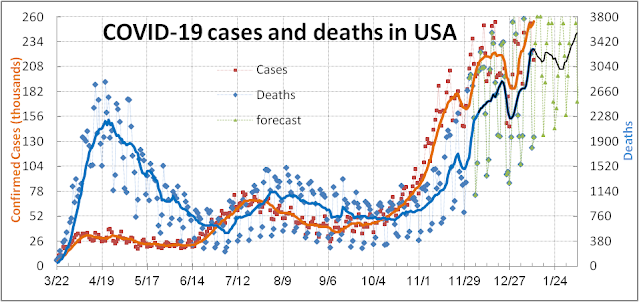
Before noon on January 20th, President Trump will leave his office. At that time the reported death toll from COVID-19 in the USA will be over 400,000 – the exact number depending on who does the tallying. Worldmeter will show 412k – real-time, Johns Hopkins will show 402k – lagging by a day, and CDC will show lower – lagging by a couple of days. All these estimates understate the real toll history will attribute to Trump – over 500k Americans died on his watch.
COVID-19 death reporting has time lags and other issues.
1. Accurately assigning the correct cause of death is sometimes more art than science. There are the underlying cause and the proximate cause issue. Sometimes COVID-19 starts a chain of events that lead to death many months later from lung, heart, kidney, liver, or diabetes problems that are not uniquely attributable to COVID-19. The US CDC separately defines confirmed and probable counts and reports both now. A confirmed case or death is defined by matching confirmatory laboratory evidence for COVID-19. A probably case is more loosely defined but is now included by most states reporting to the CDC. There is no time limitation. (Other countries use different definitions that sometimes make comparisons across jurisdictions difficult.)
2. Excess deaths, or deaths above normal average year expectations, often exceed the reported COVID-19 deaths implying that undercounting of COVID-19 deaths may be occurring using the direct method. As of Oct. 15th when reported deaths were 216k, CDC estimated excess death near 299k – 42% more.
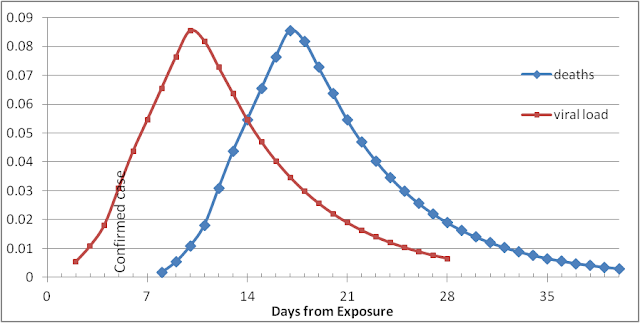
Our models for the COVID-19 virus infection and death are based on curves that rise quickly after exposure, peak, and then fall off with a long exponential tail. The virus incubates in the victim’s body and proliferates until 10 days after exposure when the viral load begins to decline in response to the body’s defenses. Those with a low overall viral load may never see a high enough load to experience any symptoms or request testing. About 10% of those exposed and get tested, typically around day 5, test positive (the current US weekly positivity rate). About half of these never develop any symptoms but carry a high enough viral load to infect others for about 10 days after test or 15 days after exposure. Half of those who test positive will usually experience some symptoms. Most will stay home and treat themselves with medical guidance. Some 6% of all positives will get sick enough to go to the hospital – although this has dropped recently to near 3%. The steady drop since August is due to more kids and young adults being positive not requiring hospitalization, but it could also be due to overcrowding of hospital systems in certain regions like Los Angeles and Arizona. About 1.5% of all those that tested positive will ultimately die in an average of 14 days from testing and 19 days from exposure. As noted above, these deaths could take up to 8 weeks to get reported and counted.
Thus when President Biden is sworn in on Jan 20th there will be:
1. Deaths that have already occurred before Jan 20th that will get reported over the following 8 weeks (35k).
2. There will be a percentage of the 3.4M cases confirmed in the period before Jan 20th that will progress to hospitalizations, ICUs, and deaths that no one will be able to save. The full accounting will take another eight weeks (69k).
3. Alternatively, by the end of March the excess death report from the CDC will provide a measure of all deaths to Jan 20th and a portion of deaths to Feb 3rd that should be attributed to Trump’s policies and actions that President Biden could not reverse (140k).
Whether using the case classification method or the excess death certificate method – the conclusion will be that more than half a million Americans died of COVID-19 under Trump’s watch that no one else could have saved. Some might argue that every country suffered from the same devastating COVID-19 pandemic – it’s not Trump’s fault. However, if Trump performed as well as the average government around the world and experienced the same average fatality per capita, only 71k Americans would have died by Jan 20th. Trump’s gross mismanagement of the pandemic will be a large part of his legacy.
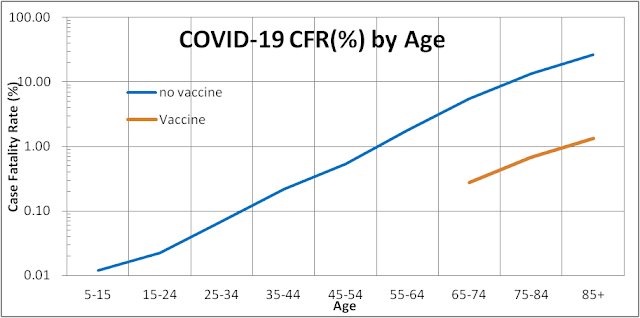
The mRNA vaccines level the playing field for older Americans. It probably doesn’t reduce your chances of being infected by SARS-CoV-2, but if and when you do, you are more likely to be asymptomatic than without it. That means you are more likely to survive the infection and your likelihood of dying from COVID-19 could decrease by roughly 95%. This will reduce the extraordinary demand for hospital and health resources. In fact, the CFR for all age groups could fall below 2%. The strong caveat though is that SARS-CoV-2 and its variants will remain highly contagious until 80% of the population is vaccinated and herd immunity is achieved.
Demand for vaccines will outstrip supply for months so I would recommend that everyone who qualifies sign up for the vaccine sooner rather than later and avoid the Florida fiasco. Moreover, releasing vaccines reserved for second doses means that inventory and distribution management will have to be extremely well-tuned to avoid missing second doses at the recommended times. This is a well-studied problem in business supply chain and inventory management. However, given the government’s track record to date, this will not be a slam-dunk.
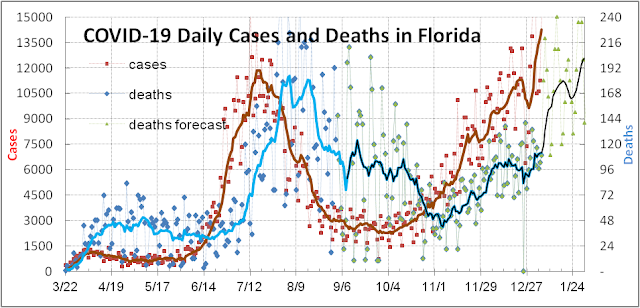
The third wave in Florida has been a little more challenging to forecast for fundamental and political reasons. The third wave in Florida began with the opening of the school year in September and began to be manifest as increased cases in early October (see figure below).
Hospitalizations began to rise two weeks later in late October (see figure below) and is now 3.66 times higher headed toward a new record.
Increased deaths did not manifest itself until early November (refer back to the first figure above). All this was predictable. The less predictable part was the longer lag time or slower transmission of the virus from kids to older adults and then to grandparents who are most susceptible to fatal outcomes (see figure below).
This last transfer did not take place in large numbers until December when the weather cooled, holiday gatherings occurred, and more activities moved indoors in Florida. The mass inoculation of seniors 65+ that just began, and the rapid spread of the B.1.1.7 variant among the young should keep the median age of infectees younger in this third wave. The net effect is to lower our expectation of the case fatality rate (CFR = cases/deaths) for this third wave to 1.6% from 2.0% for the second wave.
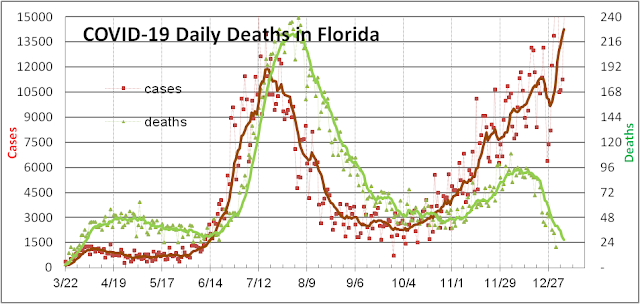
The slower than expected rise in reported death counts is also somewhat artificial due to changes in the way Florida reports deaths due to COVID-19 that stretched the COVID-19 death reporting from 2 weeks for the first wave to 2-4 weeks for the second wave to 3-8 weeks for the third wave. In the figure below, with deaths plotted against actual date, you can see that late November and December counts are still incomplete.
Recently some deaths from September finally got reported in January. We believe this is due to the FL Governor’s efforts to suppress reporting of deaths to make the pandemic seem less dangerous and justify his laissez-faire pandemic policies. Hopefully when the new administration takes office, there will be less motivation to politicize scientific data for the pandemic.
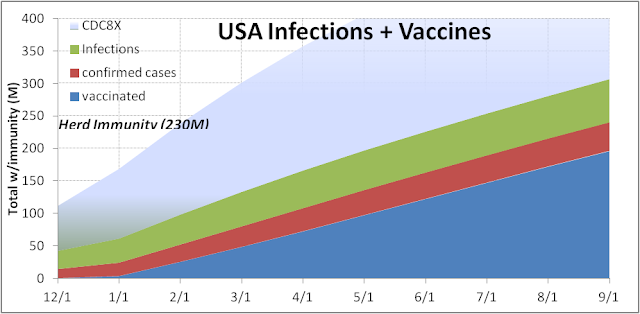
Our current forecast for Florida is that cases will peak in late January, hospitalizations will peak in early February and death counts will peak in late February or early March. With a combination of natural and acquired immunity (via vaccines), Florida could achieve herd immunity by summer and hopefully, avoid the fourth surge.