The US government’s response to the novel coronavirus has been poor from day one. And now Mark Meadows, the White House Chief of Staff says the federal government has given up trying to control the Pandemic. This admission of defeat is highly irresponsible and borders on the criminal. Governments are elected to serve and protect the people and when they fail to do their number one job, they should be voted out.
The President and his national security advisors knew in early January, and the President understood the seriousness of the novel coronavirus by late January – way before the public or other government officials knew.
(1) Even if he did not want to panic the public, he should have convened a meeting of federal officials, governors, and top local officials secretly and warned them about the coming crisis. A Manhattan Project for the Pandemic should have been set up in January to help the USA deal with this crisis. He downplayed the virus.
(2) The President should have invoked DPA (Defense Procurement Act – which he eventually did 6-8 weeks later) and made sure that the USA was prepared in terms of testing, contact tracing, quarantine facilities, hospital beds, masks, and other PPE (Personal Protective Equipment). The governors did not have this power and had to bid against one another for PPE. Kushner should not have dropped his committee work to develop more sources for PPE. Masking should have never developed into a political issue if there were no shortages.
(3) When the President found out that the CDC was poorly prepared to do testing he should have accepted Germany’s offer of a PCR test in January or bought ones from South Korea to supplement our short supply. Governors were not allowed to bypass the Federal government restrictions until mid-March. To this day Trump has an irrational ambivalence to testing. Testing and measuring is a bedrock concept in science, medicine, and even in business. You cannot fix a problem if you don’t measure and understand the full scope of the problem. Ignoring it does not make it magically go away.
(4) The President should not have politicized CDC recommendations regarding closing and reopening businesses. Governors and local officials should decide when to shutdown/reopen businesses and facilities. But national health guidelines should be available and consulted to avoided patchwork and ineffective responses and confusion. Metro-NYC pandemic cannot be managed by a single governor. When states run out of hospital beds, equipment and doctors and nurses, governors often have just the difficult choice to shut down the state or put patients out on the street. Uniform, unbiased health guidance would help in making this difficult decision.
(5) Uniform and equitable policy regarding testing, manufacturing, and distribution of vaccines and therapeutics are still lacking. Governors have to beg for Remdesivir (or Regeneron antibodies) with Trump inserting himself to play favorites – ridiculous and dangerous repeat of PPE shortage fiasco.
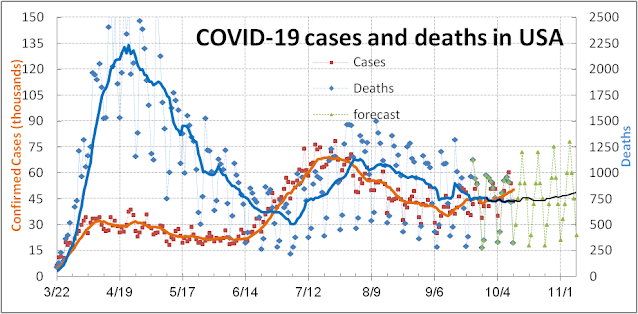
The USA has done orders of magnitude worse in this Pandemic than Taiwan, Japan, or South Korea so we know the Pandemic can be controlled. On many COVID-19 measures, the USA ranks in the top-10 worst country in the world when it should be ranked the best. 225,000 (or 300,000 if you count excess deaths) Americans need not have died. The sad thing is the USA is not much better prepared for this third attempt at controlling the Pandemic – 10 months after the first case appeared in the USA – 10 months after President Trump knew that this was a deadly disease and a serious national problem.